Clustering of 27,525,663 Death Records from the United States Based on Health Conditions Associated with Death: An Example of Big Health Data Exploration

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Definitions
2.3. Statistics
3. Results
3.1. Total Sample
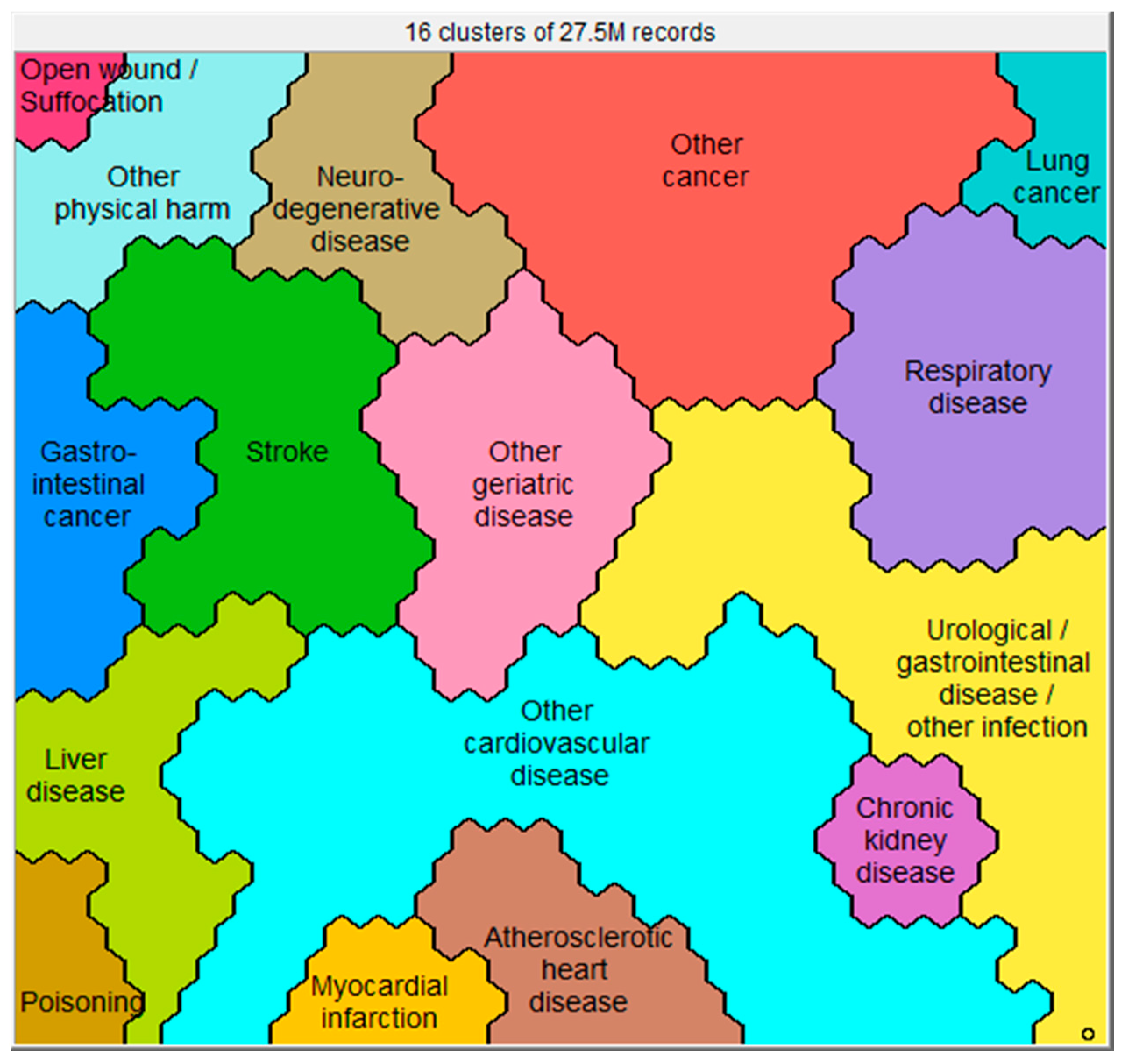
3.2. Clusters Based on the Health Conditions at the Time of Death
3.2.1. The ‘Other Cardiovascular Disease’ Cluster (n = 4,850,234)
3.2.2. The ‘Other Cancer’ Cluster (n = 3,316,586)
3.2.3. The ‘Urological/Gastrointestinal Disease/Other Infection’ Cluster (n = 3,125,752)
3.2.4. The ‘Respiratory Disease’ Cluster (n = 2,561,110)
3.2.5. The ‘Other Geriatric Disease’ Cluster (n = 1,833,980)
4. Discussion
4.1. Big Health Data Exploration
4.2. Clinical Relevance of Current Findings
4.2.1. Multiple Health Conditions Associated with Death
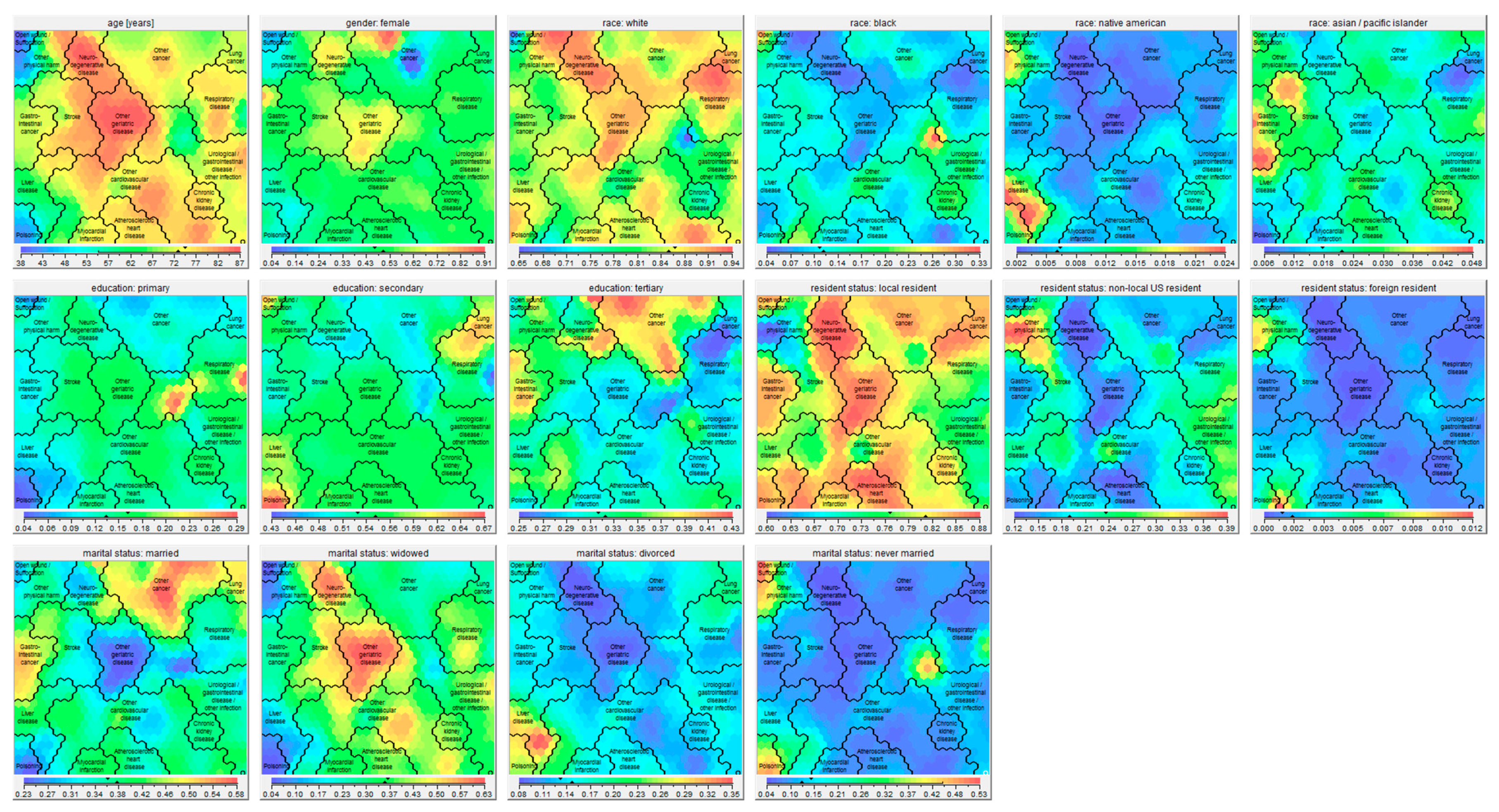
4.2.2. Dying at Old Age
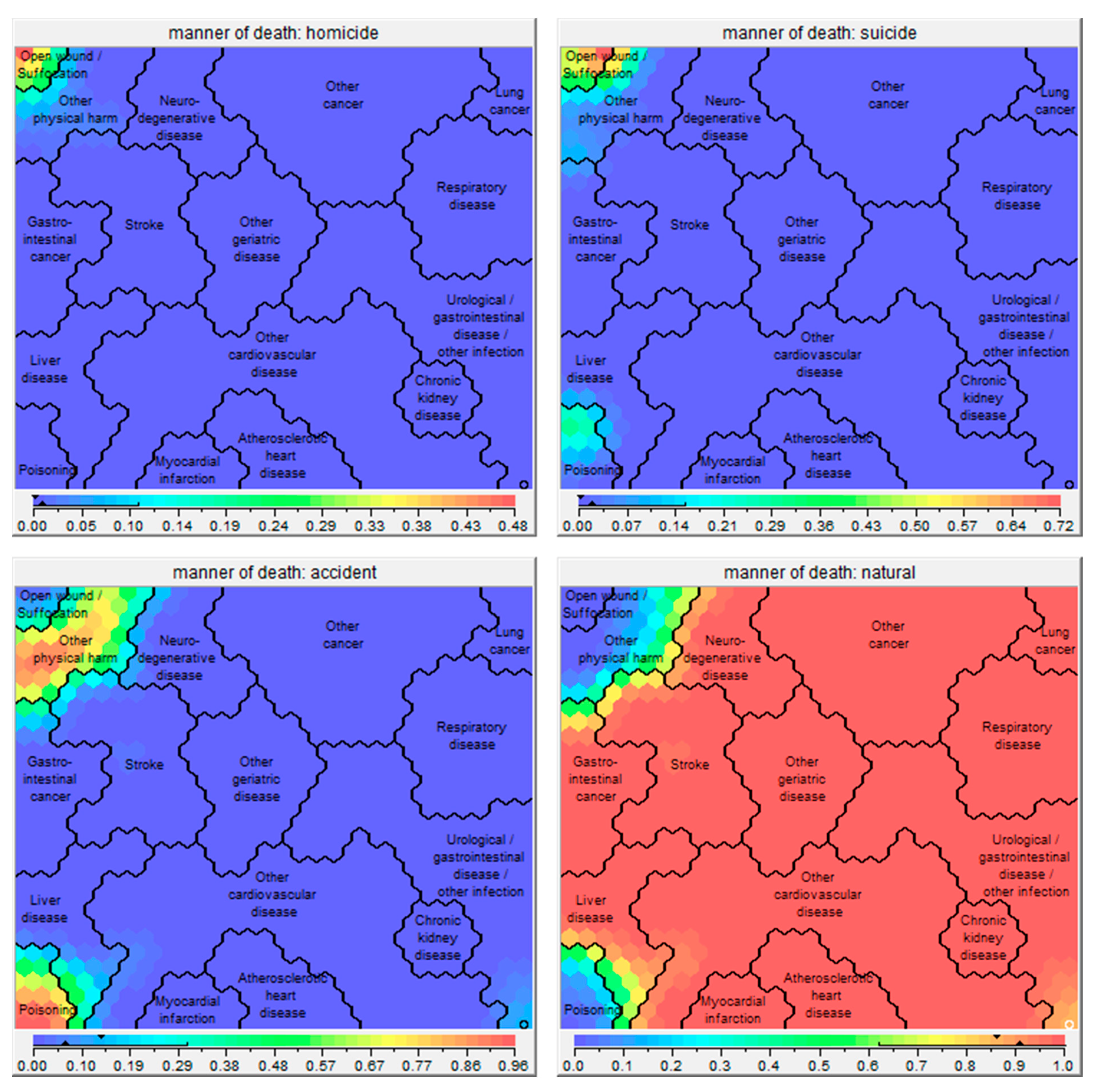
4.2.3. Dying at Young Age
4.2.4. Other Socio-Demographic Differences between Clusters
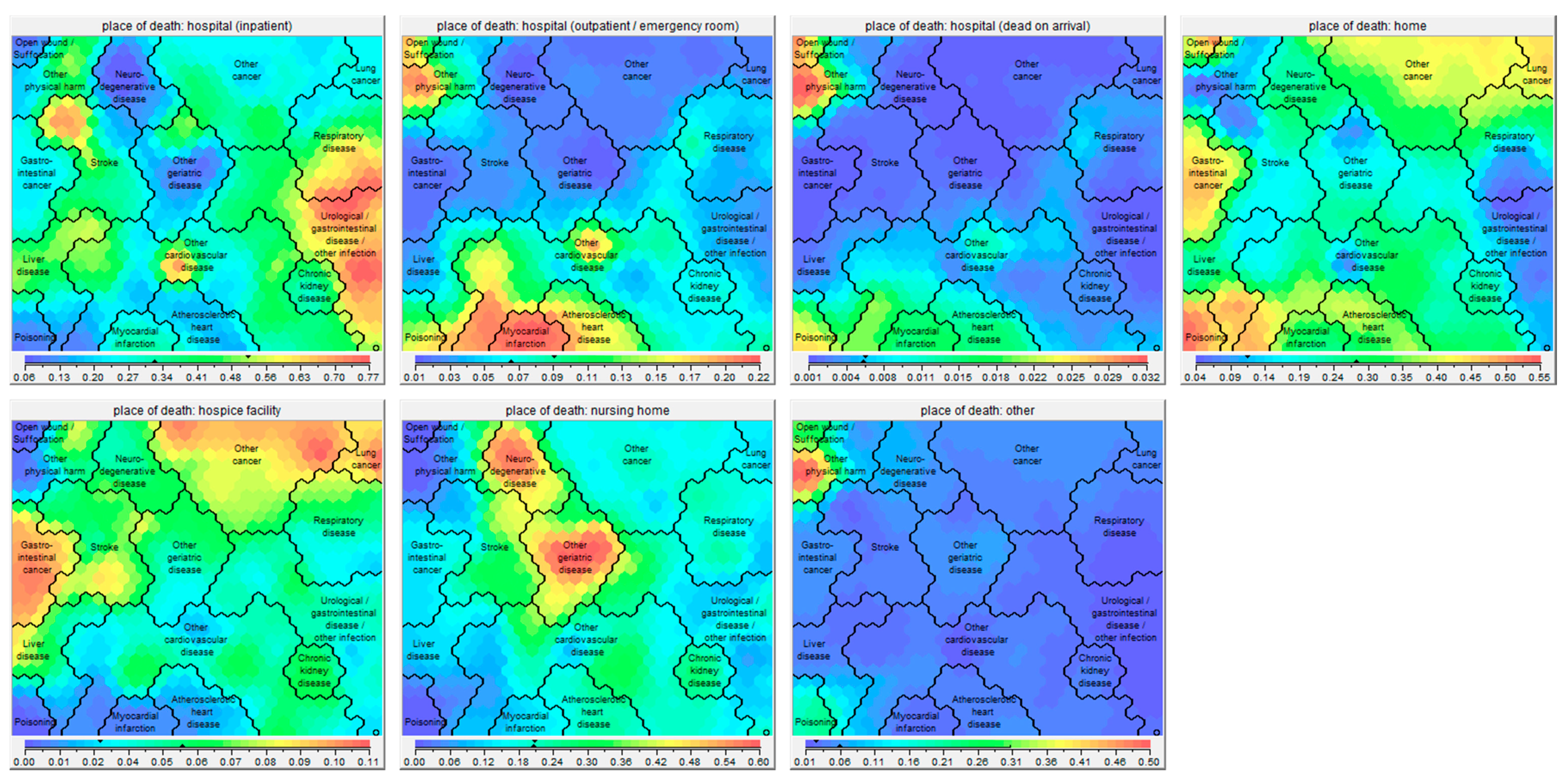
4.2.5. Place of Death
4.3. Methodological Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Okazaki, K.; Oka, N.; Shinano, T.; Osaki, M.; Takebe, M. Differences in the metabolite profiles of spinach (Spinacia oleracea L.) leaf in different concentrations of nitrate in the culture solution. Plant. Cell Physiol. 2008, 49, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Kastberger, G.; Kranner, G. Visualization of multiple influences on ocellar flight control in giant honeybees with the data-mining tool Viscovery SOMine. Behav. Res. Methods Instrum. Comput. 2000, 32, 157–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clementschitsch, F.; Jurgen, K.; Florentina, P.; Karl, B. Sensor combination and chemometric modelling for improved process monitoring in recombinant E. coli fed-batch cultivations. J. Biotechnol. 2005, 120, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Churilov, L.; Flitman, A. Towards fair ranking of Olympics achievements: The case of Sydney 2000. Comput. Oper. Res. 2006, 33, 2057–2082. [Google Scholar] [CrossRef]
- Shanmuganathan, S.; Sallis, P.; Buckeridge, J. Self-organising map methods in integrated modelling of environmental and economic systems. Environ. Model. Softw. 2006, 21, 1247–1256. [Google Scholar] [CrossRef]
- Spruit, M.A.; Augustin, I.M.; Vanfleteren, L.E.; Janssen, D.J.; Gaffron, S.; Pennings, H.J.; Smeenk, F.; Pieters, W.; van den Bergh, J.J.; Michels, A.J.; et al. Differential response to pulmonary rehabilitation in COPD: Multidimensional profiling. Eur. Respir. J. 2015, 46, 1625–1635. [Google Scholar] [CrossRef]
- Vanfleteren, L.E.; Spruit, M.A.; Groenen, M.; Gaffron, S.; van Empel, V.P.; Bruijnzeel, P.L.; Rutten, E.P.; Op’t Roodt, J.; Wouters, E.F.; Franssen, F.M. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 728–735. [Google Scholar] [CrossRef]
- Holmbom, A.H.; Eklund, T.; Back, B. Customer Portfolio Analysis Using the SOM. ACIS Proc. 2008, 5, 412–422. [Google Scholar] [CrossRef]
- Claster, W.B.; Shanmuganathan, S.; Ghotbi, N. Text mining of medical records for radiodiagnostic decision-making. J. Comput. 2008, 3, 1–6. [Google Scholar] [CrossRef]
- Heiss-Czedik, D.; Bajla, I. Using self-organizing maps for object classification in Epo image analysis. Meas. Sci. Rev. 2005, 5, 11–16. [Google Scholar]
- World Health Organization. Strengthening of Palliative Care as a Component of Integrated Treatment throughout the Life Course. Report by the Secretariat. 2014. Available online: http://appswhoint/gb/ebwha/pdf_files/WHA67/A67_31-enpdf (accessed on 14 June 2017).
- Arias, E.; Xu, J. United States Life Tables, 2015. Natl. Vital Stat. Rep. 2018, 67, 1–64. [Google Scholar] [PubMed]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- GBD 2017 Causes of death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- World Health Organization. Strengthening of palliative care as a component of integrated treatment throughout the life course. J. Pain Palliat. Care Pharm. 2014, 28, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Kohonen, T. Self-Organizing Maps, 3 ed.; Springer: Berlin, Germany, 2001. [Google Scholar]
- Kernick, D.; Chew-Graham, C.A.; O’Flynn, N. Clinical assessment and management of multimorbidity: NICE guideline. Br. J. Gen. Pr. 2017, 67, 235–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Datla, S.; Verberkt, C.A.; Hoye, A.; Janssen, D.J.A.; Johnson, M.J. Multi-disciplinary palliative care is effective in people with symptomatic heart failure: A systematic review and narrative synthesis. Palliat. Med. 2019. (In press) [Google Scholar]
- Etkind, S.N.; Bone, A.E.; Gomes, B.; Lovell, N.; Evans, C.J.; Higginson, I.J.; Murtagh, F.E.M. How many people will need palliative care in 2040? Past trends, future projections and implications for services. BMC Med. 2017, 15, 102. [Google Scholar] [CrossRef]
- Van der Steen, J.T.; Radbruch, L.; Hertogh, C.M.; de Boer, M.E.; Hughes, J.C.; Larkin, P.; Francke, A.L.; Junger, S.; Gove, D.; Firth, P.; et al. White paper defining optimal palliative care in older people with dementia: A Delphi study and recommendations from the European Association for Palliative Care. Palliat. Med. 2014, 28, 197–209. [Google Scholar] [CrossRef]
- De Witt Jansen, B.; Brazil, K.; Passmore, P.; Buchanan, H.; Maxwell, D.; McIlfatrick, S.J.; Morgan, S.M.; Watson, M.; Parsons, C. ’There ’s a Catch-22’—The complexities of pain management for people with advanced dementia nearing the end of life: A qualitative exploration of physicians’ perspectives. Palliat. Med. 2017, 31, 734–742. [Google Scholar] [CrossRef]
- Dickinson, C.; Bamford, C.; Exley, C.; Emmett, C.; Hughes, J.; Robinson, L. Planning for tomorrow whilst living for today: The views of people with dementia and their families on advance care planning. Int. Psychogeriatr. 2013, 25, 2011–2021. [Google Scholar] [CrossRef] [PubMed]
- Bauer, K.; Schwarzkopf, L.; Graessel, E.; Holle, R. A claims data-based comparison of comorbidity in individuals with and without dementia. BMC Geriatr. 2014, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- Evers, M.M.; Meier, D.E.; Morrison, R.S. Assessing differences in care needs and service utilization in geriatric palliative care patients. J. Pain Symptom Manag. 2002, 23, 424–432. [Google Scholar] [CrossRef]
- Kase, S.M.; Waldman, E.D.; Weintraub, A.S. A cross-sectional pilot study of compassion fatigue, burnout, and compassion satisfaction in pediatric palliative care providers in the United States. Palliat. Support. Care 2018, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Saeed, F.; Hoerger, M.; Norton, S.A.; Guancial, E.; Epstein, R.M.; Duberstein, P.R. Preference for Palliative Care in Cancer Patients: Are Men and Women Alike? J. Pain Symptom Manag. 2018, 56, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Noordman, J.; van Vliet, L.; Kaunang, M.; van den Muijsenbergh, M.; Boland, G.; van Dulmen, S. Towards appropriate information provision for and decision-making with patients with limited health literacy in hospital-based palliative care in Western countries: A scoping review into available communication strategies and tools for healthcare providers. BMC Palliat. Care. 2019, 18, 37. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.E.; Engelberg, R.A.; Sharma, R.; Downey, L.; Fausto, J.A.; Sibley, J.; Lober, W.; Khandelwal, N.; Loggers, E.T.; Curtis, J.R. Race/Ethnicity, Socioeconomic Status, and Healthcare Intensity at the End of Life. J. Palliat. Med. 2018, 21, 1308–1316. [Google Scholar] [CrossRef]
- Chino, F.; Kamal, A.H.; Leblanc, T.W.; Zafar, S.Y.; Suneja, G.; Chino, J.P. Place of death for patients with cancer in the United States, 1999 through 2015: Racial, age, and geographic disparities. Cancer 2018, 124, 4408–4419. [Google Scholar] [CrossRef] [Green Version]
- Kaye, E.C.; Gushue, C.A.; DeMarsh, S.; Jerkins, J.; Li, C.; Lu, Z.; Snaman, J.M.; Blazin, L.; Johnson, L.M.; Levine, D.R.; et al. Impact of Race and Ethnicity on End-of-Life Experiences for Children with Cancer. Am. J. Hosp. Palliat. Care. 2019. [Google Scholar] [CrossRef]
- Ingersoll, L.T.; Alexander, S.C.; Priest, J.; Ladwig, S.; Anderson, W.; Fiscella, K.; Epstein, R.M.; Norton, S.A.; Gramling, R. Racial/ethnic differences in prognosis communication during initial inpatient palliative care consultations among people with advanced cancer. Patient Educ. Couns. 2019, 102, 1098–1103. [Google Scholar] [CrossRef]
- Kingston, A.; Wohland, P.; Wittenberg, R.; Robinson, L.; Brayne, C.; Matthews, F.E.; Jagger, C.; Green, E.; Gao, L.; Barnes, R.; et al. Is late-life dependency increasing or not? A comparison of the Cognitive Function and Ageing Studies (CFAS). Lancet 2017, 390, 1676–1684. [Google Scholar] [CrossRef] [Green Version]
- Garlo, K.; O’Leary, J.R.; Van Ness, P.H.; Fried, T.R. Burden in caregivers of older adults with advanced illness. J. Am. Geriatr. Soc. 2010, 58, 2315–2322. [Google Scholar] [CrossRef] [PubMed]
- Riffin, C.; Van Ness, P.H.; Wolff, J.L.; Fried, T. Family and Other Unpaid Caregivers and Older Adults with and without Dementia and Disability. J. Am. Geriatr Soc. 2017, 65, 1821–1828. [Google Scholar] [CrossRef] [PubMed]
- Dionne-Odom, J.N.; Azuero, A.; Lyons, K.D.; Hull, J.G.; Tosteson, T.; Li, Z.; Li, Z.; Frost, J.; Dragnev, K.H.; Akyar, I.; et al. Benefits of Early Versus Delayed Palliative Care to Informal Family Caregivers of Patients with Advanced Cancer: Outcomes from the ENABLE III Randomized Controlled Trial. J. Clin. Oncol. 2015, 33, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.J.; Allgar, V.; Macleod, U.; Jones, A.; Oliver, S.; Currow, D. Family Caregivers Who Would Be Unwilling to Provide Care at the End of Life Again: Findings from the Health Survey for England Population Survey. PLoS ONE 2016, 11, e0146960. [Google Scholar] [CrossRef] [PubMed]
- Smith, R. A good death. An important aim for health services and for us all. BMJ 2000, 320, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Grande, G.E.; Ewing, G. National Forum for Hospice at H. Informal carer bereavement outcome: Relation to quality of end of life support and achievement of preferred place of death. Palliat. Med. 2009, 23, 248–256. [Google Scholar] [CrossRef]
- Khandelwal, N.; Curtis, J.R.; Freedman, V.A.; Kasper, J.D.; Gozalo, P.; Engelberg, R.A.; Teno, J.M. How Often Is End-of-Life Care in the United States Inconsistent with Patients’ Goals of Care? J. Palliat. Med. 2017, 20, 1400–1404. [Google Scholar] [CrossRef]
- Johnson, M.J.; Allgar, V.; Chen, H.; Dunn, L.; Macleod, U.; Currow, D.C. The complex relationship between household income of family caregivers, access to palliative care services and place of death: A national household population survey. Palliat. Med. 2018, 32, 357–365. [Google Scholar] [CrossRef]
- Murray, S.A.; Kendall, M.; Boyd, K.; Sheikh, A. Illness trajectories and palliative care. BMJ 2005, 330, 1007–1011. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.; Beernaert, K.; Van den Block, L.; Morin, L.; Hunt, K.; Miccinesi, G.; Cardenas-Turanzas, M.; Onwuteaka-Philipsen, B.; MacLeod, R.; Ruiz-Ramos, M.; et al. Differences in place of death between lung cancer and COPD patients: A 14-country study using death certificate data. NPJ Prim. Care Respir. Med. 2017, 27, 14. [Google Scholar] [CrossRef] [PubMed]
- Lobb, E.A.; Lacey, J.; Kearsley, J.; Liauw, W.; White, L.; Hosie, A. Living with advanced cancer and an uncertain disease trajectory: An emerging patient population in palliative care? BMJ Support. Palliat. Care 2015, 5, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Rietjens, J.A.C.; Sudore, R.L.; Connolly, M.; van Delden, J.J.; Drickamer, M.A.; Droger, M.; van der Heide, A.; Heyland, D.K.; Houttekier, D.; Janssen, D.J.A.; et al. Definition and recommendations for advance care planning: An international consensus supported by the European Association for Palliative Care. Lancet Oncol. 2017, 18, 543–551. [Google Scholar] [CrossRef]
- Agarwal, R.; Norton, J.M.; Konty, K.; Zimmerman, R.; Glover, M.; Lekiachvili, A.; McGruder, H.; Malarcher, A.; Casper, M.; Mensah, G.A.; et al. Overreporting of deaths from coronary heart disease in New York City hospitals, 2003. Prev. Chronic Dis. 2010, 7, A47. [Google Scholar] [PubMed]
- Ong, P.; Gambatese, M.; Begier, E.; Zimmerman, R.; Soto, A.; Madsen, A. Effect of cause-of-death training on agreement between hospital discharge diagnoses and cause of death reported, inpatient hospital deaths, New York City, 2008–2010. Prev. Chronic Dis. 2015, 12, E04. [Google Scholar] [CrossRef]
- Roulson, J.; Benbow, E.W.; Hasleton, P.S. Discrepancies between clinical and autopsy diagnosis and the value of post mortem histology; A meta-analysis and review. Histopathology 2005, 47, 551–559. [Google Scholar] [CrossRef]
- Agarwal, R.; Norton, J.M.; Konty, K.; Zimmerman, R.; Glover, M.; Lekiachvili, A.; McGruder, H.; Malarcher, A.; Casper, M.; Mensah, G.A.; et al. Do we really know the cause of death of the very old? Comparison between official mortality statistics and cohort study classification. Eur. J. Epidemiol. 2009, 24, 669–675. [Google Scholar] [CrossRef]
- Klijs, B.; Nusselder, W.J.; Mackenbach, J.P. Nationwide individual record linkage study showed poor agreement of causes of death and hospital diagnoses at individual level but reasonable agreement at population level. J. Clin. Epidemiol. 2014, 67, 160–168. [Google Scholar] [CrossRef]
- McGivern, L.; Shulman, L.; Carney, J.K.; Shapiro, S.; Bundock, E. Death Certification Errors and the Effect on Mortality Statistics. Public Health Rep. 2017, 132, 669–675. [Google Scholar] [CrossRef]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Connor, S.R.; Bermedo, M.C.S. Global Atlas of Palliative Care at the End of Life; Worldwide Palliative Care Alliance (WPCA); World Health Organization: Geneva, Switzerland, 2014; Available online: http://www.who.int/nmh/Global_Atlas_of_Palliative_Care.pdf (accessed on 7 February 2019).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Person Characteristics | n (%) or Mean (SD) |
|---|---|
| Age at death (years) | 73.12 (18.00) |
| Female | 13,697,099 (49.76%) |
| Race | |
| White | 23,533,801 (85.50%) |
| Black | 3,213,637 (11.68%) |
| American Indian | 176,329 (0.64%) |
| Asian/Pacific islander | 601,896 (2.19%) |
| Education Level | |
| Primary | 3,536,306 (13.29%) |
| Secondary | 14,546,015 (54.65%) |
| Tertiary | 8,532,106 (32.06%) |
| Marital Status | |
| Married | 10,359,202 (38.02%) |
| Widowed | 9,633,551 (35.36%) |
| Divorced | 3,930,144 (14.43%) |
| Never married | 3,320,267 (12.19%) |
| Resident Status | |
| Local Resident | 22,265,873 (80.89%) |
| Non-Local US Resident | 5,211,399 (18.93%) |
| Foreign Resident | 48,391 (0.18%) |
| Place of Death | |
| Hospital (Inpatient) | 8,929,942 (32.61%) |
| Hospital (Outpatient / Emergency room) | 1,851,801 (6.76%) |
| Hospital (Dead on Arrival) | 163,868 (0.60%) |
| Home | 7,609,594 (27.79%) |
| Hospice Facility | 1,450,220 (5.30%) |
| Nursing Home | 5,658,607 (20.66%) |
| Other | 1,722,917 (6.29%) |
| Manner of Death | |
| Accident | 1,394,442 (6.26%) |
| Suicide | 435,553 (1.96%) |
| Homicide | 201,661 (0.91%) |
| Natural | 20,243,277 (90.88%) |
| Different Health Conditions associated with Death a | 3.04 (1.83) |
| Multimorbid b | 21,579,345 (78.40%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janssen, D.J.A.; Rechberger, S.; Wouters, E.F.M.; Schols, J.M.G.A.; Johnson, M.J.; Currow, D.C.; Curtis, J.R.; Spruit, M.A. Clustering of 27,525,663 Death Records from the United States Based on Health Conditions Associated with Death: An Example of Big Health Data Exploration. J. Clin. Med. 2019, 8, 922. https://doi.org/10.3390/jcm8070922
Janssen DJA, Rechberger S, Wouters EFM, Schols JMGA, Johnson MJ, Currow DC, Curtis JR, Spruit MA. Clustering of 27,525,663 Death Records from the United States Based on Health Conditions Associated with Death: An Example of Big Health Data Exploration. Journal of Clinical Medicine. 2019; 8(7):922. https://doi.org/10.3390/jcm8070922
Chicago/Turabian StyleJanssen, Daisy J.A., Simon Rechberger, Emiel F.M. Wouters, Jos M.G.A. Schols, Miriam J. Johnson, David C. Currow, J. Randall Curtis, and Martijn A. Spruit. 2019. "Clustering of 27,525,663 Death Records from the United States Based on Health Conditions Associated with Death: An Example of Big Health Data Exploration" Journal of Clinical Medicine 8, no. 7: 922. https://doi.org/10.3390/jcm8070922